- Location: Qutub Institutional area
- Capacity: 150 patients
- Architect: Mr. Anil Yadav
- The hospital is one of the prestigious hospitals in delhi and can be said to beautifully dovetailing modern treatment with holistic healthcare.

LOCATION
- Location of the hospital should be convenient in relation to the people it serves.
- The site offer sufficient space for hospital departments.
- It is a quiet location with no possibility of future intrusive development not excluded by regulations on adjacent sites.
- The land must not be contaminated and adequate open areas for later expansion must also be planned.

ZONING
BASEMENT: OPD SERVICES RADIOLOGY LABORATORY OPD PHARMACY OFFICE
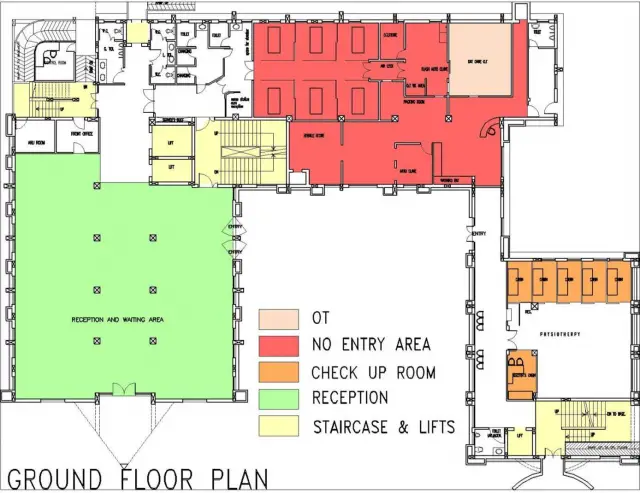
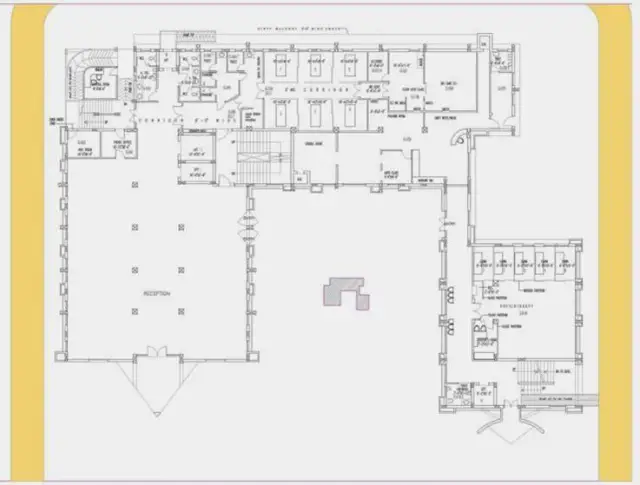
GROUND FLOOR: RECEPTION,CUM WAITING AREA, PHYSIOTHERAPY DAY CARE UNIT (OPERATION THEATRE)
FIRST FLOOR: OPERATION THEATRE, ICU, POST OPERATIVE WARDS
SECOND FLOOR: PATIENTS ROOM
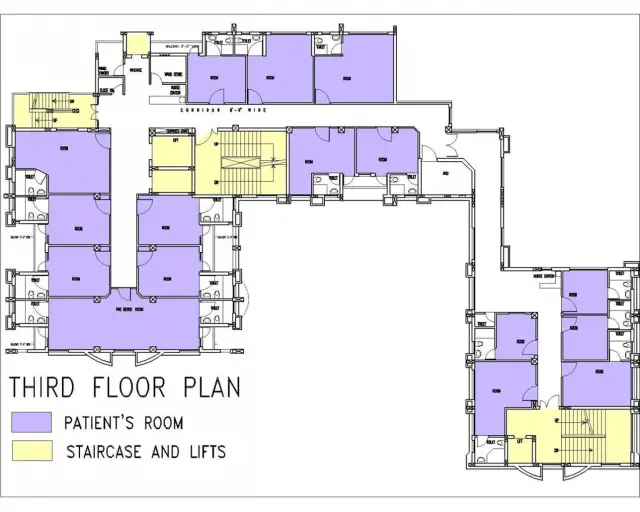
THIRD FLOOR: PATIENTS ROOM
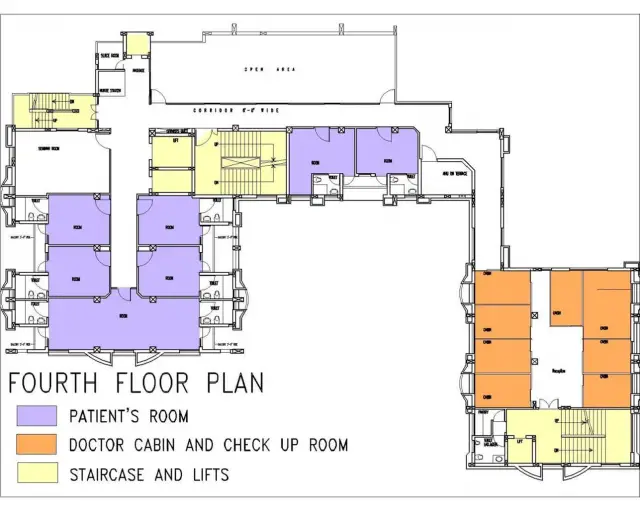
FOURTH FLOOR PATIENTS ROOM
LANDSCAPING

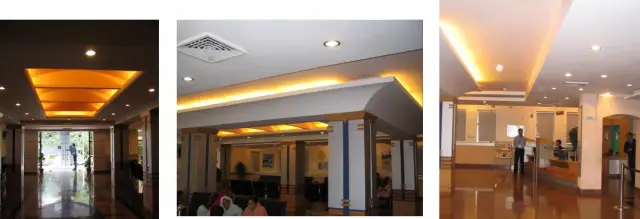
The glory of the magnificent infrastructure and the warmth of the ambience distinguish Rockland Hospital from the rest. The hospital atrium surrounded with fountains and greenery adds a soothing and healing touch of its own.
 Driveway
Driveway
CAR PARKING
- Parking being provided with in the setbacks of the hospital area mostly at the back.
- Some cars were parked in front of the hospital.
- Location of the hospital should be convenient in relation to the people it serves.
- Effective zoning is required.
- Privacy and confidentiality are important , especially at the reception desk and clinical rooms during consultations and treatments.
- Security and supervision in the premises will be necessary including staff protection against personal assault and equipment safeguarded against theft and vandalism.
- For running costs, efficient staffing , energy efficiency, long life and low maintenance approaches should be adopted.
- Flexibility and growth should be catered for flexibility in the use of some spaces, and potential for future extension of the building
STRUCTURAL
CONSIDERATIONS SUBSOIL LEVEL – Determines how heavy a structure can be erected on site.
FOUNDATION – Items as rock, water, sand, swamp, gravel, and artificial fill will determine what type of foundation is possible and appropriate. Eg. Whether basement would be risky because of water conditions or whether elevator pits would have to be blasted out because of rock presence.
PRONENESS TO EARTHQUAKES FIRE RESISTANT CLASSIFICATION – Fire and building codes specify what fire resistive type of structure like wood framed, steel , concrete structures and any combination thereof is required to meet.
OCCUPANCY CLASSIFICATION – Fire and building codes also placed restrictions on the type of structure that can be built, based on the expected occupancy of the structure.
FIRE PROOFING REQUIREMENTS – The kind of structure will also dictate the amount of water proofing to be done. Eg: what type of walls are allowed, and how many smoke barriers are necessary for each floor.
STRUCTURAL LOADING REQUIREMENTS – Structural configuration will vary considerably between an auditorium, a library, a hydrotherapy room and a row of patients.
TYPES OF STRUCTURES
The three structural materials used today are concrete, steel, and wood. each has advantages and disadvantages. each can be used alone and in conjunction with each other.
CONCRETE
(poured in place) In most cases, concrete poured in place will be reinforced concrete of either slab, columns or beams. For 1-2 storey structures, a wall bearing condition with concrete slabs and beams might be considered. Concrete has proved to be the most versatile material for health care facilities since it gives good fire proofing without additional messy material.
STEEL
A steel skeleton is the next best solution for health care facilities since it can be erected relatively fast, and it allows work to proceed quickly for other trades. However fire proofing requirements can be messy. Steel structures can be combined with concrete floor slabs of both precast and poured types.
CONCRETE (PRECAST)
The precast columns and beams with either precast slabs or poured concrete slabs can be used. Precast and pre stressed floor and roof slabs can also be used but they cannot be cut for utilities to pass through. The holes for utilities must be designed into this system.
WOOD
The wood structure is very easy to build. However, in most instances, fire safety restrictions limit the height of such a structure to a one storey, isolated building. Other fire resistive considerations are necessary such as treated wood, ceiling and partition construction. Wood is quite restricted when used for structural purposes in health care facilities because of its combustibility.
MASONARY STRUCTURE (CONCRETE BLOCK OR BRICK)
A wall bearing masonry structure might be considered for 1,2 or 3 storey structures. It can be combined with concrete slabs or precast slabs. Bothe exterior walls and interior partitions can be wall bearing. (i.e., the walls carry the load in place of beams and columns). This method is best for such buildings as nursing homes, dormitories and some utility type structures because of its cost and ease of construction.
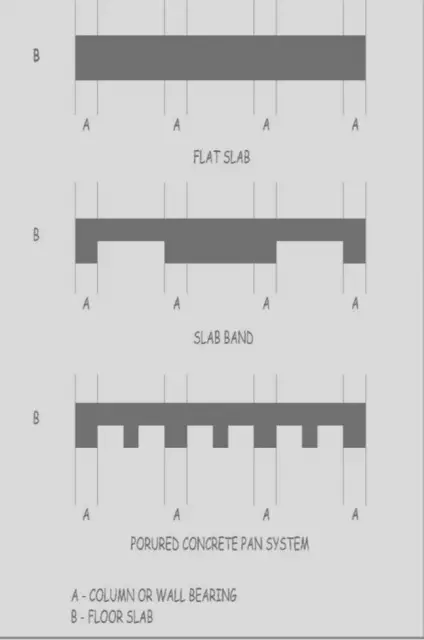
COMBINATIONS
One or more of the preceding types of structures can be combined. Figure shows some of the more common combinations used.
MAIN ENTRANCE
General traffic goes only to the main entrance; for hygiene reasons (e.g. risk of infection), special entrances are to be shown separately. The entrance hall, on the basis of the open-door principle, should be designed as a waiting room for visitors. Today’s layouts are more like that of a modern hotel foyer, having moved away from the typical hospital character. The size of the hall depends on bed capacity and the expected number of visitors. Circulation routes for visitors, patients and staff are separated from the hall onwards. The reception and telephone switchboard (12m2) are formed using counters, allowing staff to supervise more effectively. However, it must be possible to prevent public access from reception to inner areas and main staff circulation routes.
MAIN ENTRANCE WAITING AREA RECEPTION
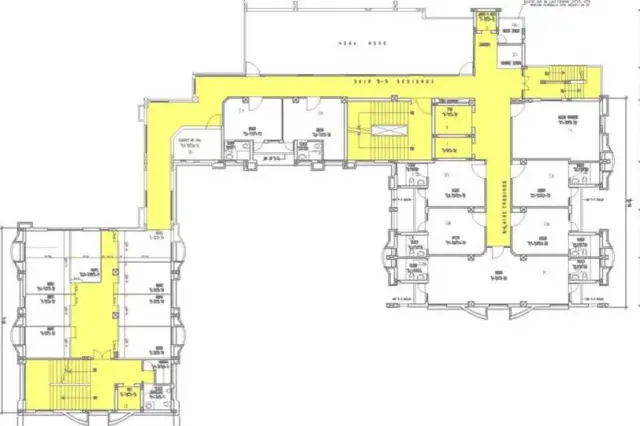
CIRCULATION
Entrance and circulation within the building must consider wheelchair users, parents with small children and people with disabilities.
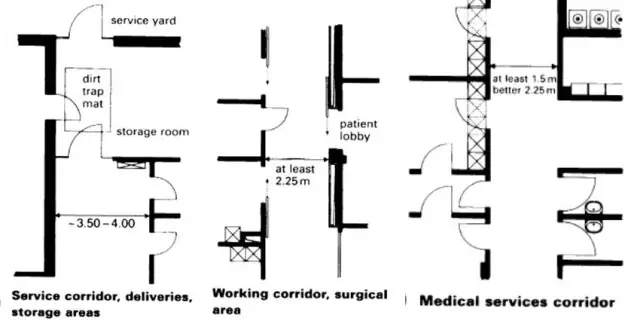
CORRIDORS
Corridors must be designed for the maximum expected circulation flow.
- Generally, access corridors must be at least 1.50m wide. corridors in which patients will be
- transported on trolleys should have a minimum effective width of 2.25m.
- The suspended ceiling in corridors may be installed up to 2.40 m.
- Widows for lighting and ventilation should not be further than 25m apart.
- Smoke doors must be installed in ward corridors in accordance with local regulations.
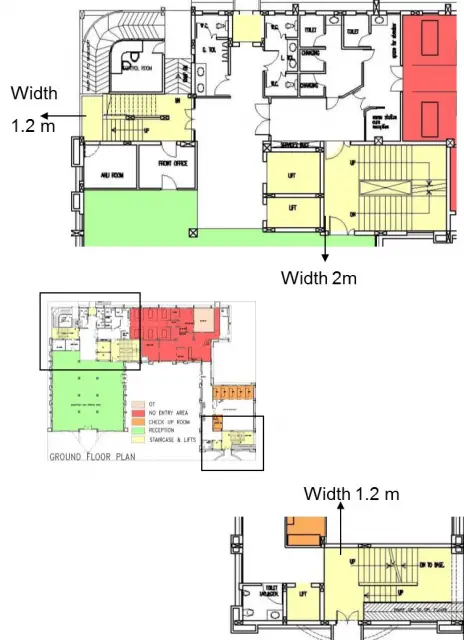
BASEMENT CORRIDORS
Extensive use of artificial light in the basement because of unavailability of natural light in the basement.
UPPER FLOOR CORRIDORS
- Artifical light not required during day time.
- Large non openable windows providing good natural light and external view . Width of access corridors 2m and 2.5 m

DOORS
- When designing doors the hygiene requirements should be considered.
- The surface coating must withstand the long-term action of cleaning agents and disinfectants, and they must be designed to prevent the transmission of sound, odours and draughts.
- Doors must meet the same standard of noise insulation as the walls surrounding them.
- A double-skinned door leaf construction must meet a recommended minimum sound reduction requirement of 25dB.
- The clear height of doors depends on their type and function: Normal doors 2.10-2.20m Vehicle entrances, oversized doors 2.50m Transport entrances 2.70-2.80m Minimum height on approach roads 3.50m
STAIRS
For safety reasons stairs must be designed in such a way that if necessary they can accommodate all of the vertical circulation.
The effective width of the stairs and landings in essential staircases must be a minimum of 1.50 m and should not exceed 2.50 m.
Doors must not constrict the useful width of the landings and, in accordance with hospital regulations, doors to the staircases must open in the direction of escape.
Step heights of 170 mm are permissible and the minimum required tread depth is 280 mm.
Rise/Tread ratio of 150:300 mm.
DIMENSIONAL CO-ORDINATION
- Modules: Modular dimensional co-ordination is the best starting point for meeting strategic design requirements. Reference systems, basic modules and multiple modules for construction details, layout and dimensions of building parts are all to be considered. For hospital construction the preferred module dimensions 12m are recommended, or 6M or 3M if the increments are too numerous. In this system all the building components are co-ordinated with each other. The supporting structure can be drawn in by producing a horizontal and vertical basic grid.
- An agreement on dimensions has considerable consequences for building construction, and the building systems available on the market must conform to this dimensional co ordination. It is therefore helpful to prescribe a normal standard dimension in planning. The benefits of dimensional co-ordination are shorter construction periods and easier replacement of interior fittings, with less disruption of service.
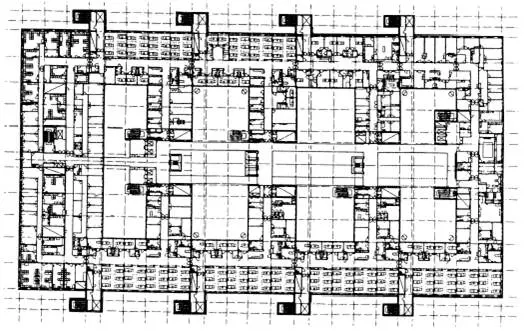
USE OF GRIDS: The Chelsea and Westminster Hospital in London is one of the largest hospitals in Europe and demonstrates how a hospital of this size can be organised and planned around a simple grid. The large internal courtyards allow natural lighting into most of the rooms on all floors. The design grid, on which all subsequent divisions are based, measures about 7.2 x 2.2m. Both the examination rooms and wards {with centres at 3.6m) are designed to comply.
MAIN SURGICAL ROOMS
- A number of necessary supply and workrooms adjoin the operating theatre directly.
- The operating theatre should be designed to be as square as possible to allow working whatever direction the operating table is turned in.
- A suitable size would be 6.50 X 6.50m, with a clear height of 3.00m and an extra height allowance of roughly 0.70m for air conditioning and other services. Operating theatres should be fitted out as uniformly as possible, in order to offer maximum flexibility, and centre on a transportable operating table system which is mounted on a fixed base in the middle of the room. The operating theatre should be connected to the anaesthetics room, discharge room, a wash room and sterile materials room via electric sliding doors, fitted on the outer side of the theatre so as not to constrict the space within. The opening mechanisms must be operated by foot switches for hygiene reasons. In the rooms for auxiliary functions, swing doors with a clear width of 1.00-1 -25 m are sufficient.
Anaesthetics Room
- The anaesthetics room should be approximately 3.80 X 3.80m in size and have electric sliding doors into the operating theatre (clear width l.40m). These doors must have windows to give a visual link with the operating theatre. The room should be equipped with a refrigerator, draining sink (sluice), rinsing line. Cupboards for cannulas, connections for anaesthesia equipment and emergency power.
- Anaesthetic discharge room
- This is set out identically to the anaesthetics room. The door to the working corridor should be designed as a swing door with a clear width of 1.25m
- Wards must have windows to give natural lighting whereas the service rooms (treatment areas, nurses’ rooms, pharmacy etc.) can be located in the artificially lit inner area.
There is a window for each bed. Size of nursing unit can vary from 20-75 beds. The nursing unit is the most important element of the many comprising the hospital. It is the space where the patient actually lives during his sojourn in the hospital.
X ray Room
Ceiling height for x ray room is 11 feet location.The most important factor that will vary the laboratory program from one hospital to another.l North orientation so as to escape the possible annoyance of direct sunlight Resilient floors acid and grease resistant.
Sterile Goods Room
The size of this room is more flexible but there must be sufficient shelf and cupboard space and it must be accessed directly from the operating theatre. One room of roughly 10m? is required per operating theatre.
Equipment Room
Although direct access to the operating theatre is preferable, it is not always feasible; where direct access cannot be provided, the equipment room must be located as close as possible to the theatre in order to reduce waiting times. A room size of approximately 20m should be allowed.
Plaster Room
- For hygiene reasons this is not located in the surgical zone but in the outpatient area. In emergencies the patient must be channelled through lobbies in order to get to the operating theatre.
- Beds must not be too close together in the recovery room and allow enough space for the anaesthetist and his equipment to reach at least three sides. Awkward additional equipment, such as sublimation stands, also requires adequate space for ease of movement. The patient is supplied via mobile service bridges with connections for a vacuum line, nitrous oxide, oxygen, power and lighting. All the necessary equipment can be accommodated in a suspended equipment trolley.
- The route between the recovery room, the operating theatre and the ward should contain several doors and be as short as possible so the anaesthetist can get to the patients quickly in case of emergency.
Recovery Room Requirements
- The recovery room must accommodate the post-operative patients from more than one operating theatre. The number of beds required is calculated as 1.5 times the number of operating theatres. Adioining is a small sluice room with drainage sinks. A nurse’s monitoring position must be provided from which all the beds can be seen. Designs should allow in daylight to help the patients to orientate themselves.
- Arrangement: The intensive care department must be a separate area, and only accessible through lobbies (for hygiene reasons). Note that according to hospital regulations, each intensive care unit must be a separate fire compartment. Apart from the patient and staff lobbies, visitors should only access the unit through a visitors’ lobby (waiting room). The central point of an intensive care unit must be an open nurses’
- workstation from which it is possible to oversee every room. The recovery room of the operating department is often located in the intensive care unit so the patients can economically be cared for by the same staff.
- The number of patients per unit should be between six and ten in order to avoid overloading the medical and nursing personnel and to provide the patient with the best possible care. One nurse’s duty station, a sterile workstation (medication and infusion preparation), one materials room and one equipment room per unit (six to ten beds) should be included in the plan.
SERVICE YARD
Hospital logistics should be centred in one place. A service yard, conveniently situated in a low-level supplies and disposal area, makes this possible. The supply and disposal of all hospital goods and materials is conducted via a separate road connection, segregated from the main and emergency entrances. During planning, consideration must be given not just to the parking and manoeuvring area for goods vehicles, but also to the wide variety of waste to be managed (kitchen, septic, metal, glass, paper, chemicals etc.) and the necessary storage requirements. In addition, service yard auxiliary rooms house emergency electricity generators, the sprinkler control room, the oxygen distribution system, and other services.
9c presentation. Cud u plz
9c presentation. Cud u plz mail me d exact presentation…In which i can view clear plans… thanku
Very informative presentation
Very informative presentation
thank u..!! it really helped
thank u..!! it really helped me for my new project..